
’Most scientists think what we’re doing is not conceivable’: Pandemic detectives on a quest for a cure
When an 18-year-old soldier tragically died in 1918, a sample of his lung tissue locked away for over a century, forgotten. A team of Brisbane-based scientists scoured the globe to find it and are now using it to supercharge the quest for a cure – before the next worldwide pandemic hits.


In a small, windowless laboratory deep inside a hospital next to the Brisbane River, a group of scientists are huddled around a large monitor, collectively holding their breath. A piece of precious lung tissue, preserved in formaldehyde and paraffin, has been sourced from a European museum where it had been stored for over a century, virtually forgotten. A sliver of the tissue – taken from the lungs of an 18-year-old German soldier who died of Spanish flu – has been prepared on a slide, and slipped under the gaze of an ultra-modern microscope. If this bold experiment comes off, it will be the first time in history that the microbiological secrets of one of the world’s most devastating pandemics have ever been revealed.
For the past hour, Dr Arutha Kulasinghe and his team have been painstakingly staining this sliver of lung tissue with over 100 colourful “markers” that bind to and identify certain proteins, attracting a cocktail of antibodies and revealing the intricate architecture of the cells within. If this experiment works, fluorescent DNA strands on the nanoscale will light up this century-old biological specimen like a disco.
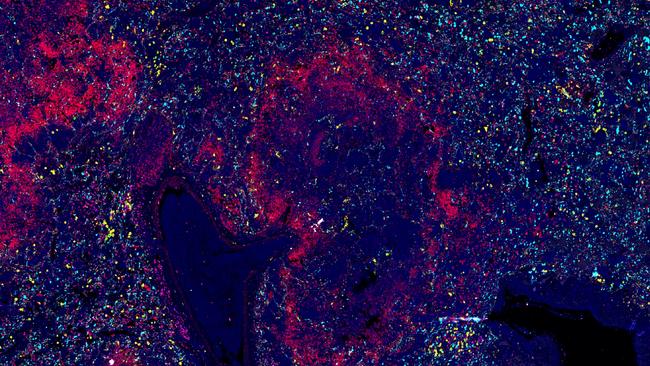
A switch is flipped on the microscope and in seconds, thousands of pink, blue, brown and green dots appear on the monitor – a kaleidoscope of cells. As those on the Zoom link squint into their screens, the jubilant exclamation of Kulasinghe punctures the pregnant silence in the stuffy laboratory and blasts through headphones across the country. “It works!” he cries. “The bloody experiment works!”
Until very recently, no scientist would have dreamt that a human tissue sample that had been out on the lab bench for even a day could be viable, let alone a piece of lung dating from 1919. But an extraordinary collaboration in Brisbane between intensivists, virologists and experts in cutting-edge digital pathology was the impetus for this bold experiment unfolding at the Wesley Research Institute.
“This is a medical Tardis moment,” says the scientific director of the project, the irrepressibly inventive Scottish-born clinician Professor John Fraser. “We’ve got a scientific time machine. To be looking back at tissue from someone that died during the Spanish flu, and to be able to tell what every cell in that tissue is doing – this is exactly like going back in time through a microscope and seeing tissue exactly as it was at the moment this poor person died 105 years ago. It’s goosebumps.”
But this scientific quest launched by the Queensland Spatial Biology Centre (QSBC) is no mere historical frolic. Having just lived through a pandemic that began without notice and brought a daily avalanche of fear, exhaustion, helplessness and sometimes grief, this team, a collaboration between St Andrew’s War Memorial Hospital and the University of Queensland, and funded by the Wesley Research Institute, is hunting through history in an effort to alter the course of the future.
“If you don’t understand the past, you’re doomed to repeat it,” says Associate Professor Kirsty Short, a virologist at the University of Queensland. “There will be another pandemic, without a doubt, within my lifetime. It’s so important that we understand past pandemics to prepare for the next one.
“What this project is doing is really going back in history to prepare for the future. And the power of that is just phenomenal.”

From the first months of Covid-19 in early 2020, then for three relentless years, like most scientists and doctors at the frontline of responding to a novel coronavirus, Short worked long hours attempting to understand the nature of SARS-CoV-2 (the virus that causes Covid-19), the wide plethora of effects it had on the body’s systems, and how it might be treated. Scientific understanding of Covid-19 developed relativly quickly amid extraordinary worldwide collaboration. Vaccine science catapulted forward at warp speed. Yet still, treatments remained elusive. Even in the modern metropolis of New York City, ambulances containing refrigerated bodies lined the streets, unable to offload the victims to overloaded morgues. To date at least seven million people worldwide have died of Covid-19, and still there’s little remedy at hand. Mass mortality was not the only devastation: the pandemic brought the world economy almost to its knees, triggering one of the largest global economic crises since the Great Depression. Travel ceased, and airlines went bust as their planes sat idle; India burned its dead in collective pyres. Children experienced social and academic isolation during the formative years of their lives. The elderly in nursing homes spent countless months locked away from their families, many simply perishing from loneliness.
As Australia shut borders and then locked down in the early months, Fraser – Director of Intensive Care at St Andrew’s War Memorial Hospital, and Director of the Critical Care Research Group at The Prince Charles Hospital – found himself in the discombobulating position of having no patients across the Brisbane public and private hospitals he worked within, but a flood of reports and panicked updates from the world’s worst-hit hotspots, from Italy to Brazil. With the virus spreading fast around the world, Fraser co-founded the Covid-19 Critical Care Consortium, headquartered in Brisbane, an international research and data-sharing group assembled to harness the cumulative experience of intensive care units worldwide.

The response by medical science to the Covid-19 pandemic came at a time in history when technology was already rapidly transforming the fields of immunology, genetics, digital pathology and cell biology. As the virus spread across borders and millions fell sick, doctors were sharing clinical information in real time as the world united to learn all it could about this novel coronavirus. As deaths mounted, scientists began sending tissue samples from victims by courier and by post to their international colleagues with special expertise.
“Being a doctor during Covid-19 was petrifying,” recalls Fraser. “This was a brand new thing. There were lots of human jigsaw puzzle pieces of data coming in. And all the doctors were just desperate. People were phoning each other and sending each other WhatsApp messages because there was no instruction book. We didn’t know what we were doing. It was a brand new virus, and there was no vaccine.
“It was a little bit like driving down the highway at breakneck speed with a blindfold on – we knew that we didn’t have the information to go on. We had no roadmap. We normally have a rough idea of how to manage severe illness by first principles. We had a massive responsibility, but people were dying in our hands and we were helpless. When patients die, you take it home. You don’t leave it at the door.”
Even as a vaccine hit chemists in lucky countries, in terms of treatments there was very little progress made as the pandemic wore on. Monoclonal antibodies were developed, but remained expensive and inaccessible for most. The old drug dexamethasone was also repurposed as a crude remedy for hyperinflammation – one of the hallmarks of the body’s response to SARS-CoV-2. As immune cells flood the victim’s lungs to fight the virus, the body over-reacts, triggering in some individuals what’s known as a cytokine storm – a systemic inflammatory syndrome that can be life-threatening or deadly. It’s hyperinflammation that often kills patients with Covid-19.
Now, with predictions of a 70 per cent chance of a pandemic in the next 25 years killing 10 million people or more, the QSBC team is determined that doctors will never again fly so blind. Being able to map the pathophysiology of the Spanish flu in mind-boggling detail is extraordinary in itself, but that’s not the endgame for this highly unusual cross-disciplinary experiment. The vision of these Australian scientists is much greater. They’re on a quest to ensure no doctor or nurse will ever again have to hold the hand of a ventilated patient as they lie slowly dying, with no panacea and scant hope, isolated and alone.
You might call this crack team – led by Fraser, spatial biologist Kulasinghe and virologist Short – forensic biologists, or even pandemic hunters. If that’s what they are, their most important foot soldier is 29-year-old PhD student Lauren Steele, who was analysing host responses to severe disease when the pandemic hit. In August 2022 Steele flew to Vienna to meet the curator of Austria’s renowned Natural History Museum, the Naturhistorisches Museum Wien. The institution was one of several that had replied affirmatively to an email from her asking if they possessed preserved lungs or lung samples of people who were likely to have been victims of a pandemic.
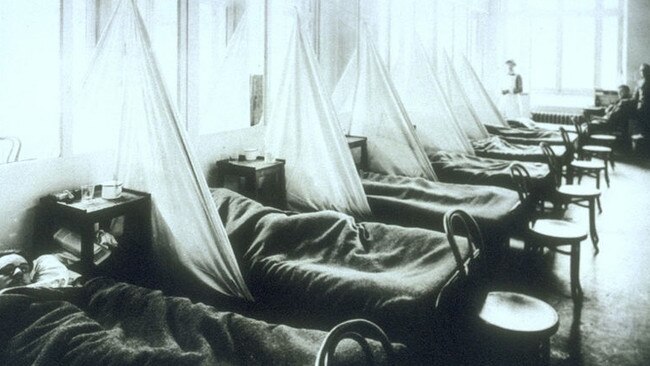
Steele was interested not just in the Spanish flu, which erupted in 1918 and quickly spread during the final stretch of World War I amid mass troop movements, raging until 1920, but also the flu pandemics of 1957 and 1968. The Spanish flu killed an estimated 50 million people worldwide, disproportionately the young. At the time it wasn’t even understood to be a virus. A bacterial cause was widely suspected, and people turned to all manner of bizarre remedies – even drinking snake oil, bloodletting and inhaling gas fumes – to try to ward off the terrifying illness.

When Steele arrived at the Vienna museum, the curator explained that the organs it held were kept in the nearby University of Vienna. But the records weren’t up to date and they didn’t really know what they had. Some samples were whole lungs fixed in formaldehyde sitting forlornly in jars; others were formaldehyde-fixed, paraffin-embedded tissue boxes stored in archives. At the University of Vienna there were two and a half rooms full of lungs. Steele spent days scouring the museum database, which tracked dates of death, to isolate potential pandemic victims, and then cross-checked any samples that possibly related to a pandemic illness against handwritten autopsy records held in enormous bound book volumes. Many of those who died of flu throughout much of the 20th century were marked as having succumbed to pneumonia, bronchitis or grippe, the earlier French descriptor for flu. “One of the samples labelled the cause of death as ‘cheesy, gelatinous pneumonia’,” Steele says. “There were some very descriptive terms.”

At the end of the Vienna detective work, Steele had identified two certain pandemic victims, with the museum agreeing to provide her with a small slice of those preserved lungs, as well as arranging ethics approval. In the meantime, the team in Queensland had gained agreement to obtain slices of tissue from two Spanish flu victims held by a German genetics researcher who had also obtained lung samples via the Berlin Museum of Medical History.
When Steele returned home, she discovered to her amazement that a museum in Sydney, the Ainsworth Interactive Collection of Medical Pathology, held a preserved lung of an Australian Spanish flu victim, a young WWI soldier, along with 15,000 other tissue samples that Steele spent weeks sorting and cross-checking against autopsy records in a dusty inner city attic, netting further precious slices of pandemic tissue.
“We’ve had four pandemics now since the [beginning of the] 20th century,” she says. “And we can kind of see patterns that happen within them. But nobody has been able to answer the questions before about the how and why.”
After Steele had returned home from Europe, Kulasinghe – who with his colleagues at the Frazer Institute across the Brisbane River had already amassed a sizeable Covid-19 biobank of tissue samples – swung into action. Kulasinghe was the key local figure with expert knowledge in the cutting-edge field of spatial omics, an emerging method of digital pathology in which unique neighbourhoods of millions of cells and their interactions with pathological biomarkers can be mapped in astonishing three-dimensional detail.
“Generally, when you cut tissue and leave it on the bench, it oxidises and it’s destroyed – it generally doesn’t preserve over time,” says Kulasinghe. “If you go into a pathology bank or a hospital, tissues are generally kept for about 10 years and thrown away.
“It should not be possible to get signal off 100-year-old tissues. Most scientists think what we are doing here is not conceivable. Running this experiment live, we’re seeing what a disease that is 100 years old did to people’s bodies, for the first time. It is incredible.”
The power to travel back in time via next-generation microscopy has its genesis in an innocuous-looking blue and white machine that sits in the corner of the QSBC lab. The device was recently purchased by the Wesley Research Institute, which realised such technology could bring together the power of its significant stores of clinical data paired with its trove of pathology specimens amassed over the course of the Covid-19 pandemic.
The million-dollar machine, dubbed the PhenoCycler, enables what is known as spatial phenotyping of countless cells at an unprecedented scale and speed. It augmented the work in this emerging field by Kulasinghe, who had set up a spatial biology lab at the Frazer Institute. Spatial biology is a new field of research which allows scientists to map cells within tissue in a level of detail and complexity that is revolutionary for science. Millions of cells can be mapped in vivid 3D detail from a single specimen slide, not only individually but also in terms of their cell neighbourhoods – or how they communicate with each other. Further, complex cell interactions can now be plotted against pathological biomarkers such as a virus, giving unprecedented insight as to how the body reacts to a particular pathogen.
Without technology like this, it is impossible to understand the three-dimensional relationships of cells and other processes occurring in the tissues, such as inflammation, which is a key factor in pandemic illnesses. Through a process of staining and “barcoding” individual cells and molecules, scientists are able to build a three-dimensional picture of an immune battlefield. As many as 100 different elements – cells, molecules and other tissue elements marking out the inflammatory battlefield – can be individually identified, yielding 3D images rich in detail.
What has never been appreciated about this cutting-edge application of spatial biology until now is that it could be used on organs soaked in formaldehyde and sitting in jars, or tissue samples stored for decades in museums.
“We realised during Covid, we were shipping tissues around at room temperature, just sending slides around the world,” Kulasinghe says. “And we were getting really good signal. Kirsty [Short] came to us and said, ‘Look, here’s a crazy idea – we’ve got this collaboration in Europe and these tissues that have been collected from 1918. Can we get signal?’ I knew the instruments we now have use a different chemistry, which allows us to look at degraded samples. So I was like, ‘Hold on, let’s just give it a go’.”
But it’s not the machine alone that provides the critical insights. A team of cross-disciplinary experts including immunologists, virologists and computational analysts must interpret the images via painstaking scientific work. Some things are immediately apparent, though. In this first look at the lung tissue of the young German soldier who contracted Spanish flu, it’s clear from the intense clusters of a type of immune cell called macrophages that crowd the image that this was a patient who experienced a hyperinflammatory immune response within his lungs shortly before dying.
The key now is to work out which exact alveolar cells or structures were infected by the 1918 influenza virus, and then to overlay that with the types of immune cells that rushed to the body’s defence. If this can be established, the exact mechanism of the body’s immune response can be ascertained. When compared to other known pandemics, if similarities in the body’s immune response are found to exist, as suspected, it will form the basis for the world’s first evidence-based understanding of the host response to pandemic illness, and how that differs between age groups; it will also give key clues as to how drugs may provide a remedy.

It’s been postulated for many decades that hyperinflammation characterised the lungs’ response to Spanish flu. But the theory has always been a hypothesis largely based on anecdote.
“A lot of the 1918 information has just come from personal diaries and people’s accounts,” Short says. “Those lived experiences are obviously very powerful. But to understand something mechanistically you need more than that. So these tissue sample images really take things from conjecture to evidence-based.
“I guess one of my fundamental hypotheses is that in 1918, you had this hyperinflammatory response in young individuals. So we can see that straight away on our images. But we can now go into so much more detail. We can quantify the cell types. We can quantify which one of those inflammatory cells is producing each inflammatory molecule – because coming up with a therapy might not be about blocking that cell, it might be about blocking the inflammatory molecule that it produces in that cell-to-cell interaction.
“So maybe it’s about one specific immune cell rushing into the lung, and then interacting with another one, and that causing an inflammatory storm. It’s about understanding the detail to ensure that any target that we find is really valid and robust.”
Halting the hyperinflammation process is the endgame of this whole endeavour – a panacea for every pandemic. If the QSBC team can identify similarities in the immune response that are replicated across pandemics, whether the virus is influenza or a coronavirus, it may be possible in the next pandemic to develop a universal therapy that could protect the population, especially young people who are often wiped out in the largest numbers in pandemics (Covid-19 was an anomaly in this regard; it largely killed the elderly). Such a therapy may be in the form of an antibody injection that could block a particular target cell type or signalling molecule in order to prevent the overactivation of the immune system.
As the team narrows focus to a pandemic panacea, they are tantalisingly aware that the scope of what spatial biology technology could assist scientists to do could be limitless.
“What we have done here defies the dogma,” Short says. “I think what could flow from this project would be a new dogma for what is and is not possible with tissue analysis.
“If this works on 100-year-old tissue, maybe it works if we got tissue from somebody who died during the plague; maybe it even works on the ancient Egyptians. It just opens up a whole new area of scientific discovery.”

Kulasinghe says tissues probably have to have been preserved in formaldehyde to be viable for analysis. That’s been standard practice for only about a century. But the scope to re-open clinical trials and subject stored tissues to new, much richer analysis in cancer, neurodegenerative disease and countless other conditions is vast. “It’s not just about 1918, this opens up the whole hospital pathology biobanking system, which has been keeping tissues in [formaldehyde] for hundreds of years,” he says. “We can go back to a clinical trial that might have been run for breast cancer 10 years ago that had exceptional responses to chemotherapy. And we can go pull those tissues, and we can ask the question, ‘What is in this patient cohort that defined sensitivity to a drug that might be 20 years old? And what can we learn from that?’ We’ve never pushed the boundary this far.”
Fraser, incidentally, is travelling to Egypt later this year. “Serendipity is this wonderful word in medicine,” the professor says. “Penicillin was discovered by a Scotsman by mistake, Barry Marshall discovered Helicobacter pylori bacteria by mistake. But it’s not a mistake, it’s just that these people work the hardest. And the more work you put in, the luckier you get.
“Could we find things out from the ancient Egyptians? Who knows? Could we have a Jurassic Park moment, like the mosquito that got preserved in amber? I don’t know, but I would not be averse to speaking to the Egyptian government when I’m over there in September. Never accept ‘no’ until you’re proven wrong.”
More Coverage



To join the conversation, please log in. Don't have an account? Register
Join the conversation, you are commenting as Logout