Gender fix locks future identity, say senior psychiatrists
Psychiatrists have raised ethical and scientific concerns about a treatment study of transgender-identifying teenagers and children.

Senior psychiatrists have gone public with ethical and scientific concerns about Australia’s first long-term treatment study of transgender-identifying teenagers and children.
The Trans20 study at the Royal Children’s Hospital in Melbourne involves a projected 600 patients aged 3-17 given pro-trans “gender affirming” care, including potentially sterilising hormonal treatment for gender dysphoria, or distress about one’s body.
“There’s a kind of assumption that the gender affirming treatment being provided is the gold-standard, appropriate treatment,” Sydney psychiatrist Roberto D’Angelo told The Weekend Australian.
Dr D’Angelo is one of six psychiatrists to put their names to a letter in the journal BMJ Open. “Are families actually told, ‘we’re still not sure this (affirmative model) treatment is the best way to treat gender dysphoria’?”
There is concern about possible social contagion in rapidly increasing numbers of teenagers, chiefly girls, declaring trans identity with no childhood hint of gender confusion, and undergoing novel treatments with puberty-blocker drugs, cross-sex hormones and sometimes surgery.
Critics say the evidence for these treatments is low-quality, short-term, flawed or missing.
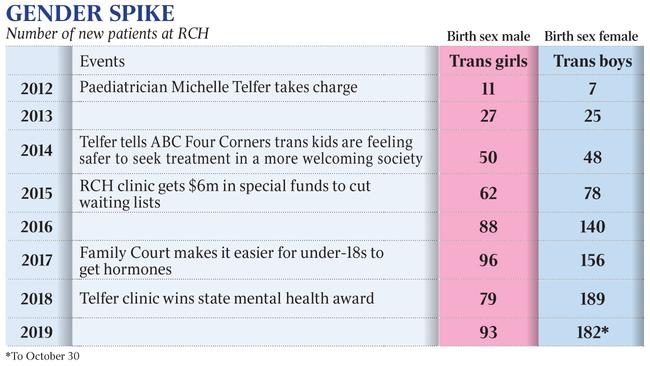
At the RCH youth gender clinic, the number of female-born new referrals in 2018 was 2600 per cent higher than in 2012 when there were just seven, according to data obtained under FOI legislation. Biological boys were up by 618 per cent.
Clinic director Michelle Telfer, a paediatrician, has appealed for more public money so RCH can begin “gender affirming surgery” (double mastectomies) for post-pubertal “transmasculine” patients.
In December, RCH chairman Rob Knowles, a former health minister, and chief executive John Stanway issued an open letter defending the Telfer clinic as “one of the world’s best”.
“The treatment we deliver on a daily basis is based on the best available medical evidence and in line with international best practice,” the letter says.
“Gender dysphoria is a recognised medical condition with a debilitating impact.
“Children with this condition are entitled to the best available medical care and we will not shy away from delivering that care.
“In doing so, we adhere to strict clinical governance standards.”
In their journal letter, the six psychiatrists say they have “grave reservations about the ethical underpinnings and methodology” of the RCH Trans20 study based on what’s been made public.
They call for the release of details showing that informed consent for participation in the study takes account of mounting concerns about the safety and ethics of the affirmative model and life-altering medical interventions.
Trans20 researcher Ken Pang said there was a response coming to the psychiatrists’ questions.
Meanwhile, in a sign of international networking by critics of the affirmative model, seven Swedish physicians, including adolescent and child psychiatrist Sven Roman, have written to Scott Morrison, backing local calls for an independent inquiry. A medical college is already reviewing standards of care.
The Swedish doctors cite the high rate of psychological and other disorders in the mostly teenage girls now diagnosed with dysphoria by gender clinics.
“There is a possibility that the majority of patients in the new group have autism or autism-like conditions,” they say.
“In their teens, people with autism have even more concerns about their body and identity than other adolescents.”
They say these patients often suffer from self-harming, eating disorders, mental trauma, depression and emotional instability, which along with autism may be the main underlying problems.
The concern is that an already vulnerable group of young people may not get the right treatment in gender-focused clinics, resulting in regret and harm.
Like similar “affirmative model” research projects in Britain and the US, the Melbourne Trans20 study lacks a comparison group of patients getting rival treatment such as cautious psychotherapy, casting doubt over what the results might mean.
“If the kids do seem better after a year or two, we won’t know whether it’s because of, or despite, the gender-affirmative intervention, or because they got a lot of attention,” Dr D’Angelo said.
Time’s cure
Before the 2000s, gender dysphoria typically appeared in preschool boys, and in most cases resolved itself as children grew up, with many emerging as young gay or bisexual adults at peace with their biological sex.
The Australian psychiatrists’ letter warns that the affirmative-only approach, with early pro-trans intervention, may “lock” young people into gender dysphoria, as well as “closing them off to future choices in identity”.
In a BMJ Open paper on their study last year, Trans20 researchers acknowledge trans youth medical treatment was “relatively new”.
They state the need for “stronger evidence (on) the natural history of gender diversity”, citing research showing that up to 88 per cent of non-gender conforming children came to embrace their biological sex as they grew up.
Critics of the affirmative model highlight this body of research showing the “desistance” of gender dysphoria — seemingly a self-correcting process involving time, growing maturity and sometimes psychotherapy — as an argument against risky medical intervention.
Whether or not the dramatic desistance rates of early-onset children apply to the new fast-growing group of teen-onset patients is an “urgent clinic issue,” according to Canadian psychologist Ken Zucker, a world authority on gender dysphoria and editor-in-chief of Archives of Sexual Behavior.
In their journal letter, the group of Australian psychiatrists express puzzlement about how the Trans20 study can discover anything about the condition’s natural history when it proposes to intervene “in the developmental trajectories of all 600 expected participants.
“We already do possess good data on the ‘natural history’ of gender confusion which shows that a majority of children desist at puberty and return to a gender identity congruent with their natal sex. Is this fact presented to concerned families?”
Go early, or not?
The 2018 treatment standards for gender dysphoric youth issued by Dr Telfer’s RCH clinic — and praised by Victoria’s Andrews government as the “world’s most progressive” and “most stringent” — do not mention the desistance phenomenon.
In their paper, the Trans20 researchers play down the desistance literature, suggesting it understates the likely persistence of gender dysphoria.
They rely on a 2018 article, by Temple Newhook et al, which complains desistance research is used as “the scientific rationale for discouraging social transition (living as the opposite sex) for pre-pubertal children.
“The tethering of childhood gender diversity to the framework of ‘desistance’ or ‘persistence’ has stifled advancements in our understanding of children’s gender in all its complexity.”
The Trans20 researchers do not cite Dr Zucker’s 2018 rebuttal of the Temple Newhook paper, in which he suggests they cherry-picked from the desistance literature, misrepresented it, and at one point fell back on “rhetoric and dogma”.
Dr Zucker’s Toronto clinic regarded gender identity in young children as far from fully formed, and as a first step tried psychosocial therapy to ease the distress of children felt in their bodies.
The clinic took a cautious approach to social transition, carried out key desistance research and was targeted by trans radicals.
Practitioners critical of the affirmative model believe early social transition — sometimes enabled by parents and schools, as well as by gender clinics — makes desistance less likely, setting some children on a path towards unnecessary medical treatment bringing with it infertility, impaired sexual function and lifelong dependence on the health system.
In his rebuttal paper Dr Zucker says it is “astonishing” the Temple Newhook article warns that discouraging social transition is itself an intervention that can affect the outcome of research, while failing to acknowledge that precisely the same should be said of encouraging social transition.
Dr Zucker says the article’s “implicit message” seems to be: “Research on persistence and desistance should be suppressed: it should just disappear without a trace.
“This is empirical and intellectual ‘no platforming’ at its worst. I find this ominous, but not surprising.”
On the desistance issue, this newspaper sought comment from Dr Temple Newhook, Dr Telfer and Dr Pang, who is a biomedical researcher and paediatrician with dual appointments at the Murdoch Children’s Research Institute and RCH.
‘Awful’ terms
In a 2018 Joy 94.9 radio interview, Dr Telfer was asked about the “80 per cent desistance myth” being used to oppose “gender affirming treatment” because trans-identifying children would “grow out of it anyway”.
She agreed there were “major problems” with the research and although not all these previous outcome studies should be put “in the one basket”, there was a “pathologising element” to the desistance literature.
“Even the terms ‘persistence’ and ‘desistance’ are pretty awful terms … it really does make one sound right and one sound wrong,” Dr Telfer said.
“Times have changed a lot and we are now taking an approach where we listen to the child and we listen to the adolescent … and support them, so they feel comfortable in identifying how they feel they are, and this wasn’t the case if you go back 20-odd years ago when Zucker first started studying this.
“Our current experience is that it is the vast majority (of young people in the RCH clinic) who will persist.”
Of 710 patients diagnosed by the clinic with gender dysphoria from 2003-2017, 96 per cent “continued to identify as transgender or gender diverse into late adolescence”, RCH told the Family Court in the 2017 case re Kelvin, which made it easier for under-18s to get cross-sex hormones.
“No patient who had commenced (cross-sex hormones) had sought to transition back to their birth assigned sex. No longitudinal study is yet available,” the judgment says, relying on evidence from RCH.
The court justified changing the law and relaxing its supervision of treatment decisions for minors by citing “advances in medical science” to do with better understanding of gender dysphoria, its affirmative treatment, and the risks of withholding or denying that treatment.
The affirmative model offers a stark choice between “life-saving treatment” and the risk of attempted suicide.
Urgent advice
In August 2019, following this newspaper’s coverage of concerns about the safety and ethics of trans youth medicine, Health Minister Greg Hunt requested urgent advice from the Royal Australasian College of Physicians.
“It is important that we have a nationally consistent standard of care that is evidence based and with appropriate safeguards to protect the interests of the patient,” Mr Hunt said.
In its open letter, RCH says it “looks forward” to the RACP’s national review of treatment.
Just before Christmas, Mr Hunt’s spokesman said the RACP’s “full review” of treatment for gender dysphoria in youth would give “objective evidence-based advice to the government and the Australian community on how this sensitive issue should be managed clinically”.
He said the college was expected to report to the government “in the coming months”.
In 2015 Dr Telfer and the RACP lobbied for easier access to “gender affirming” hormones for adolescents.
The RACP declined to comment on this potential conflict of interest.
Critics of the affirmative model including Western Sydney University’s professor of paediatrics John Whitehall and former University of Sydney psychology professor Dianna Kenny have argued for a wide-ranging federal parliamentary inquiry.
In their letter to Mr Morrison and Mr Hunt, the group of Swedish physicians recommend investigation by “an independent third party, with special competence in the evaluation of scientific evidence (and) completely free from personal or professional conflicts of interest”.
Add your comment to this story

Ley’s Liberals rebuild with a network of allies
Sussan Ley will draw on a network of top female business chiefs and counsel from long-time backers and party elders as she attempts to rebuild the decimated Liberals | See the power circle.

Riches prove we were right on CFMEU: Burke
Tony Burke says CFMEU officials could have controlled $310m in assets, saying an audit exposed serious risks that justified government’s intervention.
To join the conversation, please log in. Don't have an account? Register
Join the conversation, you are commenting as Logout